
 Español
EspañolDr. Dustin Sulak
The dosage is the key factor to achieve the greatest benefits and the least adverse effects of cannabis. After following thousands of patients who used medicinal cannabis for eight years, I have observed that the dosage cannabis is unlike any therapeutic agent I was exposed to in my medical training. A basic understanding of key features Cannabis dosage can help you make the most of this plant incredibly versatile, safe and effective.
Some patients effectively use small amounts of cannabis, while others use incredibly high doses. I’ve seen adult patients achieve therapeutic effects with 1 mg of total cannabinoids daily, while others consume more than 2,000 mg a day without adverse effects. And although a range 2000 times dosing is unusual for a drug, the researchers haven’t killed monkeys at even 300 times higher doses than the highest dose I have seen in the clinic.
Relations multiphasic dose-response
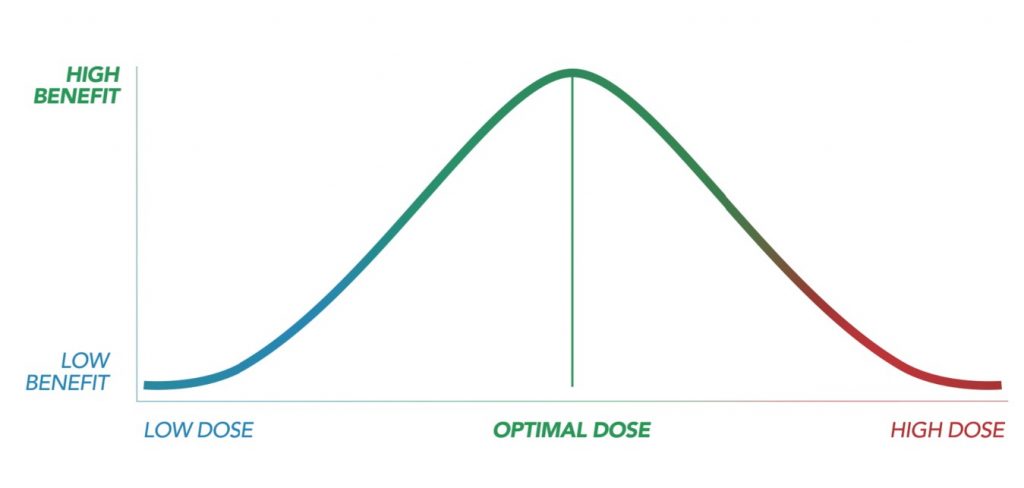
Within this unusually wide dosage range, cannabis exhibits a relationship unusual between dose and expected response. For most of the medications, a higher dose will result in a more therapeutic effect strong and a greater probability of adverse effects; this is described as a monophasic dose-response relationship. Cannabis just doesn’t follow this Pattern.
For the majority of cannabis users, gradually increase their dose by principle will have stronger effects; but after a certain point (exclusive of each individual), subsequent dose increases may have effects increasingly weak therapeutic, accompanied by an increase in the non- desired.
Consumers who continue to increase their dose to very high levels can often regain some or all of the benefit previously lost, and sometimes find additional therapeutic effects that are not achieved at the lower doses. Por supuesto, las dosis ultra altas son mucho más caras y generalmente producen más efectos secundarios no deseados. A la mayoría de los pacientes les va mucho mejor con la dosis efectiva más baja.
For many cannabis users, this means that less can be more. In a study of 263 cancer patients treated with opioids with poorly controlled pain, the group receiving 21 mg of THC and CBD combined each day experienced significant improvements in pain levels, more than the group receiving 52 mg per day. The group receiving 83 mg daily reduced their pain no better than placebo, but experienced more adverse effects.
How is this possible? The endocannabinoid system is a highly adapted and sensitive physiological infrastructure designed to maintain balance at the cellular level. When cannabinoid receptors are overstimulated with high doses of cannabis, the cells attract the receptors inward, where they are recycled or degraded. As cannabinoid receptor levels decrease, the effects of cannabis will also decrease, even (or especially) with dose escalation. This is known as “tolerance development,” something that many regular cannabis users have experienced.
Therapeutic window
The term “therapeutic window” describes the range between the lowest effective dose and the dose that produces unwanted or intolerable side effects. People with little or no experience of using cannabis often have a very narrow therapeutic window, while regular users develop a wider therapeutic window. This is due to the fact that people develop tolerance to the various effects of cannabis at different speeds, and most develop tolerance to the unwanted effects faster than the desired effects.
Bidirectional effects of cannabis
Cannabis also has the ability to produce opposite (or bidirectional) effects in different people, with different strains, and in different doses. For example, anxious people who take cannabis can relax while non-anxious people who take the same dose can become anxious. The same dose of two different varieties of cannabis can cause opposite effects: one can be an awakening strain and the other could make you sleepy.
Interestingly, the symptoms of a cannabis overdose reflect the symptoms one would expect cannabis to alleviate at the appropriate doses: nausea, vomiting, diarrhea, sweating, spasms, tremors, anxiety, panic attacks, paranoia, incoordination, and sleep disturbances. Extreme overdoses can lead to hallucinations and even acute psychosis.
Fortunately, these symptoms are self-limiting, and most people return to their normal state in 12 to 24 hours. Although a cannabis overdose can make a person feel like they are dying, such an experience will not cause toxicity or permanent harm, except perhaps in people who have unstable cardiovascular or psychiatric conditions, or in the event of a disability leading to a accident.
Combining CBD and THC
CBD and THC have many overlapping therapeutic qualities, including pain relief, anxiety, seizures, and nausea, although they work through different mechanisms of action. When combined, CBD and THC can enhance the benefits of each other while reducing the unwanted effects, including the psychoactive or harmful effects of THC. This is great news for cannabis users who want health benefits while maintaining optimal performance at home or work.
By adding CBD to THC, the therapeutic window, described above, becomes even wider. However, consumers should know that the total dose of cannabinoids needed to treat a symptom or condition will also increase.
For example, in a study of 177 patients with cancer pain, one group received a THC oral spray, while another group received a combined THC and CBD oral spray in a ratio of approximately 1: 1. Both groups were given he allowed his dose to be gradually increased until they experienced satisfactory relief. The THC group ended up using an average of 27 mg daily, while the CBD + THC group used about 60 total mg daily, but the CBD + THC group had a greater reduction in pain. I suggest this to many patients: Combine CBD and THC for optimal benefits, but be prepared to take higher overall doses.
Ultra low dose
Some patients do well with ultra high doses (hundreds or thousands of milligrams daily). THC users have to work slowly to reach these high doses, but many patients can quickly reach high doses of CBD without adverse effects. On the other hand, ultra low doses can be extremely effective, sometimes even more than the other extreme.
Most people are surprised to learn that the therapeutic effects of cannabis with dominant THC can be achieved in lower doses than required to produce euphoria. Cannabis microdosing, taking a non-psychoactive or slightly psychoactive dose in order to improve health and productivity, has been gaining popularity.
People report better mood, reduced anxiety, improved focus, increased stress resistance, less pain (and / or less bothersome pain), and other benefits without adverse effects. Most consumers find that 1-5mg works well for this purpose. Some emerging evidence even suggests that a practice like this could be protective against damage from a heart attack or brain injury.
Recommendations for new and experienced consumers
For new cannabis users, I adhere to an old adage I learned from one of my geriatric instructors: “Start low, go slow, and don’t be afraid to go all the way.” I developed an easy-to-follow program to help you find your optimal dose, along with other helpful resources, such as a medicinal cannabis shopping guide, available for free at Healer.com.
For existing users who may have developed a certain tolerance for cannabis, I encourage you to try my 6-day awareness protocol, which has helped thousands of people reduce their cannabis dose by 50% or more while improving benefits. If you have not tried non-inhaled administration methods such as tinctures or sprays, and if you have not experimented with the combination of CBD and THC, I suspect that both efforts will help you continue to unlock all the power of this amazing plant. Posted by Leafly in February 2018
References
·Thompson GR, et al. Oral and intravenous toxicity of Δ9-tetrahydrocannabinol in rhesus monkeys. Toxicology and Applied Pharmacology. 1974;27(3):648-665.
·Portenoy RK, et al. Nabiximols for opioid-treated cancer patients with poorly-controlled chronic pain: A randomized, placebo-controlled, graded-dose trial. The Journal of Pain.2012;13(5):438-449.
·Hsieh C, et al. Internalization and recycling of the CB1 cannabinoid receptor. Journal of Neurochemistry. 1999;73(2):493-501.
·Johnson JR, et al. “Multicenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain.” Journal of Pain and Symptom Management.2010;39(2): 167-179.
·Waldman M, et al. An ultra-low dose of tetrahydrocannabinol provides cardioprotection. Biochemical Pharmacology. 2013;85(11):1626-1633.
·Johnson-Sasso CP, Kao D, Walker LA. marijuana use and short-term outcomes in patients hospitalized for acute myocardial infarction. Journal of the American College of Cardiology.2016;67(13):569.
·Fernández-Ruiz J, Moro MA, Martínez-Orgado J. Cannabinoids in neurodegenerative disorders and stroke/brain trauma: From preclinical models to clinical applications. Neurotherapeutics. 2015;12(4):793-806.
·Nguyen BM, et al. Effect of marijuana use on outcomes in traumatic brain injury. The American Surgeon. 2014;80(10):979-983.
·Di Napoli M, et al. Prior cannabis use is associated with outcome after intracerebral hemorrhage. Cerebrovascular Diseases. 2016;41(5-6):248-255.